In less than a dozen years, stunning growth has changed East 105th Street, where Cleveland’s University Circle and Fairfax neighborhoods meet. Transportation access to this booming area has improved but still lags Downtown Cleveland’s even though University Circle’s employment and population are quickly catching up (Google). CLICK IMAGES TO ENLARGE THEM.
UC workforce rivals Downtown’s, access lags
AN OPINION COLUMN
Each morning, the red lines appear on the traffic app’s map. The lines, along with their yellow brethren, make for a colorful mosaic along the otherwise green-shaded grid of neighborhood streets surrounding the Cleveland Clinic. But that’s the only attractive thing about them. No one wants these indicators of traffic congestion — not city officials, Clinic officials, neighbors or commuters.
But it’s likely going to get worse.
Two parking garages are to be constructed over the next year on the Clinic’s main campus. A visitors’ garage will rise at 10681 Carnegie Ave. and an employees’ deck will be built at 8501 Carnegie Ave. Together, their 1.3 million square feet will accommodate up to 4,000 vehicles.
They will cost the Clinic $170 million to build and millions more to depreciate, operate and maintain each year.
The Cleveland Clinic is inexorably growing. Its next wave of Main Campus development looks to be even larger than its last, now wrapping up. It is adding thousands of new jobs to the city’s University Circle and Fairfax neighborhoods. The Clinic is already Ohio’s largest employer.
Neighborhoods closest to the Clinic like University Circle, Fairfax, Hough and Glenville are experiencing new investment, infill housing and growing populations — some for the first time in decades. The Clinic’s growth is undoubtedly one of Cleveland’s greatest success stories.

Every weekday morning, traffic on the four-year-old Opportunity Corridor backs up heading into University Circle. The growing district and its traffic keep on growing (NEOtrans).
But those trends are already adding indicators of growing pains that grow more acute with each new addition. At some point, an asset to the community becomes a liability when its growth is not managed carefully and thoughtfully with respect to its surroundings.
That point appears to be nearing. Clinic traffic has been clogging old arteries like MLK Drive for a long time. A new bypass of busy Chester and Carnegie avenues, the $330 million Opportunity Corridor, was crowded the day it opened in 2022 and its back-ups have intensified.
Motorists search for more fluid capillaries via residential side streets, with traffic sometimes preventing residents from getting out of their driveways, or making their ways in a timely manner to drop kids off at school and/or to get to work.
Some residents recently complained about those situations at a public meeting organized by Council President Blaine Griffin of Ward 6. They also lamented that their kids aren’t safe walking to school at the John Hay Campus or the Cleveland School of the Arts. It’s not because of urban crime. It’s because of traffic.
Many motorists who are seeking optional routes are regular commuters to the Clinic. And some of them park on those streets in defiance of signs that warn against parking there for more than two hours. Many are ticketed. They keep coming.
Griffin has repeatedly complained to Clinic officials about this quality of life issue for his constituents. There isn’t much they can do on a day-to-day basis. So the burden of the Clinic’s growth, not the just benefit, falls on the city to manage.

Cranes over the Cleveland Clinic have been a common sight in recent years. And they’re due to come back again this winter and possibly grow larger in numbers than the Clinic’s last building boom seen here several years ago (ClevelandSkyscrapers.com).
Griffin wants the Clinic to keep growing, as we all do. He also wants his residents to have peaceful neighborhoods, as we all do. Those goals are on a collision course. “This is a long conversation with several moving parts,” he told NEOtrans.
Last week, Cleveland Clinic was sent a basic premise of what this opinion column would say. They responded with the following written statement:
“Cleveland Clinic recognizes that growth at our Main Campus brings both opportunity and responsibility. Planning is coordinated with the City of Cleveland and informed by community input, with careful consideration of traffic, access and neighborhood impacts,” the Clinic said.
“The planned parking structures will reduce on-street parking and improve access for patients, visitors, and caregivers,” it continued. “We remain committed to balanced growth and will continue working with city and community partners to support access to care while being mindful of surrounding neighborhoods.”
University Circle Inc. and Fairfax Renaissance Development Corporation are also engaged in this conversation along with city officials. The problem is that the Cleveland Clinic’s Main Campus is car-dependent. It is addicted to cars in part because Clinic and city officials believe there is no other realistic solution.
Like a person dependent on a chemical to feel normal, it will probably bargain with its addiction before taking more serious, transformational actions. Every city in the USA goes through this process before making impactful, albeit costly choices at a scale similar to those that got them addicted in the first place.

University Circle has become Cleveland’s second downtown and is growing so much that it may eclipse Downtown Cleveland in employment and residents in a few years. Yet it lacks the transportation access capacity of Downtown, threatening to choke off its continued growth (Noah Belli).
The Clinic and the city may try to influence its traffic by dabbling with transportation demand management systems. Those include things like informational displays along roadways to guide traffic to more free-flowing routes. Or have smart parking garages that display the number of available spaces. Or provide incentives to share rides.
Those look good on PR materials and may address traffic at the margins. But they don’t address the underlying cause. At some point the city and Clinic are going to have to come to grips with the fact they lack a balanced transportation diet. They need to diversify. They can’t rely on just one modal food group to nourish itself.
Two such modes are walking and biking. As noted earlier, housing investments are happening around the Cleveland Clinic’s Main Campus. One of the biggest development districts in Greater Cleveland is called Circle Square, located between Euclid and Chester avenues, just east of East 105th Street.
It has added since 2023 more than 500 housing units in 11-story and 23-story buildings. Another 23-story building is in the works, adding 281 apartments. Across Euclid, in 2020, the 20-story One University Circle delivered 276 apartments. A block south of that, Skyline on Stokes added 263 units last year.
It’s an impressive list of additions. And there are more coming, adding hundreds of apartments per year. But it’s not enough. The traffic is still coming.
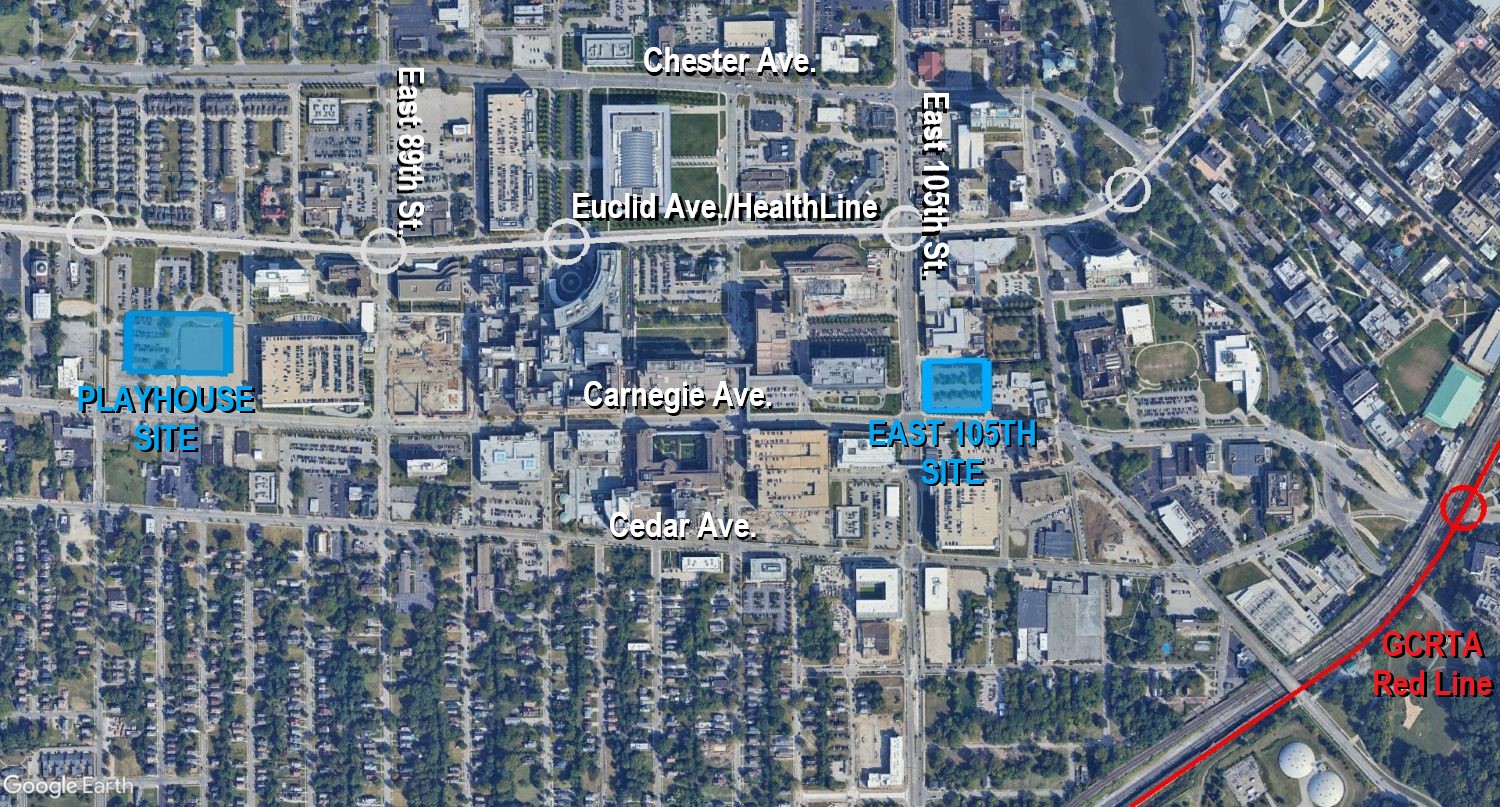
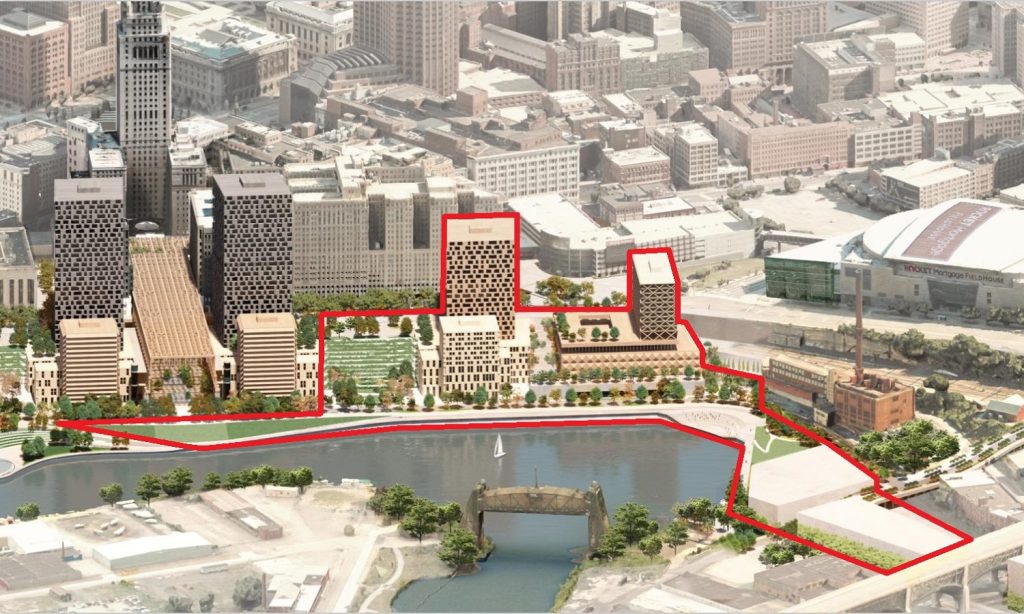
The Cleveland Clinic is building two new parking garages on its Main Campus. Demolition of the Carnegie Imaging Center at Carnegie Avenue and East 105th Street will start in the coming weeks to make way for the 1,500-space East Garage. It will be followed by the West Garage at Carnegie and East 86th Street, on the former Cleveland Playhouse site that may also host significant new Clinic facilities (Google).
To offset the need for the number of parking spaces in the Clinic’s two new parking garages would take more than a dozen of these big new apartment buildings at a construction cost of about $600 million. Remember that cost figure.
That’s how huge the new traffic burden will be, to say nothing of what’s already clogging University Circle’s roads. That doesn’t mean you don’t build the housing and provide pedestrian- and bike-friendly infrastructure. But the burden can’t rest on any one delivery system.
That includes public transportation which, despite the growth in and near University Circle, hasn’t added any new capacity this century. In fact, it has actually decreased.
The $200 million HealthLine bus rapid transit opened in 2008, replacing the No. 6 bus that operated every six to 10 minutes, not counting the Nos. 7X, 8, 9X and 32X routes from the Heights to Downtown along the so-called Dual Hub Corridor that had 53,000 weekday riders in the mid-1980s.
Bus trip times from East Cleveland to Downtown were reduced by the HealthLine from 44 minutes offered by the No. 6 to as little as 39 minutes now, but some rush-hour runs take 43 minutes. Today, the HealthLine operates every 15 minutes and carries about 5,000 riders per day.
Red Line trains and Blue Line trains share the same tracks along East 105th Street, into the heart of University Circle including to the front doors of the Cleveland Clinic Main Campus in the near future. It follows a decision by Greater Cleveland to pursue an investment in a Rapid Redesign, reconfiguring the region’s rail transit for the transportation needs of today and tomorrow (NEOtrans).
The Greater Cleveland Regional Transit Authority (GCRTA) doesn’t have the money to operate more frequent bus service to University Circle or anywhere else. In fact, it’s cutting service once again, as it has done several times so far this century. Although, GCRTA has made every effort to find other budget cuts that limit the service cuts.
To make a difference transit-wise will be expensive. University Circle and Cleveland Clinic and the city don’t need cosmetic Band-Aids like a few buses from a suburban park-n-ride delivering a few dozen people per vehicle. They need hundreds of people per vehicle coming every few minutes to make a difference in the traffic congestion.
To do that, GCRTA needs to offer a new high-capacity transit route that can carry thousands of new riders each day to the front doors of the largest traffic generators in the district. That route needs to be a frequent bus or rail rapid transit service with a dedicated right of way that keeps the transit vehicles out of the car traffic.
University Circle, Ohio’s fourth-largest employment district, does have one rail transit line — the Airport-Downtown-Windermere Red Line. But it misses the Cleveland Clinic’s Main Campus, skimming along the edge of the district.
Because of that, Clinic officials don’t consider this resource when making decisions about transportation access. Even the 2015 $900 million plan to extend the Red Line to Euclid that would have boosted ridership by 11,000 riders per day was not embraced by the Clinic because its route is too far away.
Despite nearing the employment and residential numbers of Downtown Cleveland, at upper-left, University Circle (orange circle) and the Cleveland Clinic Main Campus (light-blue circle) lack the roadway and rapid transit access of downtown (Google).
Meanwhile, Downtown Cleveland, which has bled office workers since long before the pandemic, has rail lines fanning out in four directions from Tower City Center — five if you include the mothballed Waterfront Line.
Downtown offices aren’t coming back, especially with AI suppressing office demand further in non-tech markets. GCRTA needs to adapt by redeveloping its rail station park-n-ride lots with structured parking, housing, retail and services. And one of downtown’s rail lines needs to be rerouted to University Circle.
I vote for rerouting the Blue Line from Shaker Heights. But even if the Clinic reallocated money from constructing a future parking garage to leverage federal funds for rerouting the Blue Line to its front door, GCRTA lacks the money to afford maintaining the addition of several route-miles to its 33-mile rail system.
A solution is to reroute the Red Line too — but share a portion of its realigned route miles with the rerouted Blue Line. GCRTA considered rerouting the Red Line through the heart of University Circle in its Dual Hub Corridor plans of the 1980s and 90s.
Of course, it also considered keeping the Red Line on Euclid all the way to Downtown. Doing that today would cost far too much money so a more modest concept shown in the maps and renderings in this column offers a Rapid Redesign that keeps the rail system at 33 route-miles and doesn’t add new operating costs.
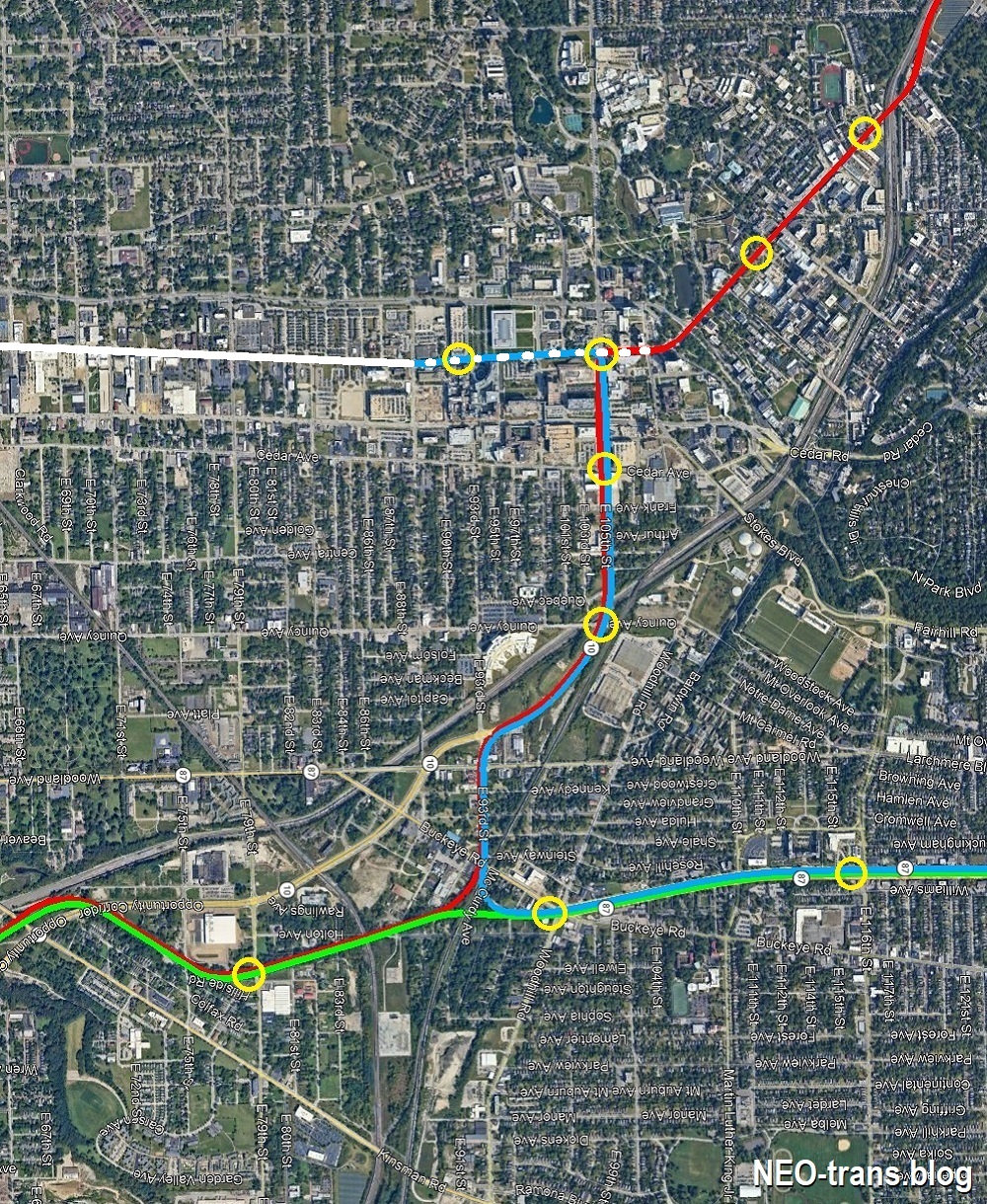
This scenario provides better rail rapid transit access to University Circle and the Cleveland Clinic’s Main Campus without adding new rail route-miles or operating costs to the Greater Cleveland Regional Transit Authority (NEOtrans).
But even that won’t be cheap. At the low end, its construction cost could equal the $500 million which the Ohio Department of Transportation expects to spend to ease Deadman’s Curve on the Inner Belt portion of Interstate 90.
At the high end, the cost could equal Cleveland Clinic’s recent tax-break-to-community-benefit-spending deficit, according to a report by the Lown Institute, a think tank that studies hospital systems.
It said the Clinic received $611 million more in tax breaks than it spent on charity care and community investment. The Clinic counters that its tax breaks allows it to employ 1,500 more people than it could otherwise afford.
Any rail line relocation or new-construction idea scares GCRTA staff and some board members. They’ve doubted their own ability to raise that kind of money. It’s part of the reason why they waited so long to replace its fleet of aging rail cars — because some at GCRTA, including former General Manager Joe Calabrese, doubted they could find $250 million.
Instead, GCRTA did something truly remarkable. They engaged in a Rapid Reboot — retrofitting the rail system with a standardized fleet of light-rail cars and modified stations and maintenance facilities for them. Starting next year, any GCRTA train can use any rail line, offering some intriguing possibilities — including this Rapid Redesign.
With the Red Line rapid transit to be converted to light-rail next year, it offers the opportunity to redesign a portion of the rail system to better serve Greater Cleveland’s fastest-growing employment hub before it chokes on its own traffic congestion (NEOtrans).
To reboot the Rapid, GCRTA raised $450 million — including the largest single grant, $130 million, it had ever received in its five-decade history. It showed GCRTA could raise big money for a big, transformative project that excited prospective funders.
Now GCRTA is engaging in a strategic planning exercise to identify risks, goals, shortcomings and opportunities to guide decisions over the next four to five years. Given its flat revenues, among the options it will consider is a sales tax increase to support the existing system albeit with some modifications.
To win support for any new revenue streams, it will need to excite and inspire the community — and to show it can also match new revenues, especially tax revenues, with other sources of investment.
If GCRTA committed an amount, say $25 million raised from leasing its park-n-rides to developers, to pursue a Rapid Redesign in the University Circle area, it could leverage larger contributions from a variety of partners. And not just the Cleveland Clinic, but the city of Cleveland through a tax-increment financing district, the Ohio Department of Transportation and the Federal Transit Administration.
What is certain is that a growing, car-dependent Cleveland Clinic will increasingly collide with its surrounding community. Its time to step up the construction of housing within walking/biking distance of the Clinic and put high-capacity public transportation at the Clinic’s front door in a creative manner that can be fiscally sustained. We must. The stakes are too high for us not to.
END